Prolonged Electrical Muscle Stimulation Exercise Improves Strength And Aerobic Capacity In Healthy Sedentary Adults

After a brief introduction on Electrical muscle stimulation methodology and applications in competitive sport for
Prithwish Banerjee,1 Brian Caulfield,2 Louis Crowe,3 and Andrew Clark1
1Department of Academic Cardiology, Castle Hill Hospital, University of Hull, Cottingham, Kingston-upon-Hull, United Kingdom; 2School of Physiotherapy and Performance Science, University College Dublin, Belfield, Dublin 4, Ireland; 3Biomedical Research Ltd., Galway, Ireland Submitted 17 August 2004; accepted in final form 18 July 2005
Electrical muscle stimulation (EMS) can be applied with a variety of protocols and parameters. Typical settings of EMS exercise involve the application of electrical stimuli delivered in intermittent trains through surface electrodes positioned over the muscle motor point and preprogrammed stimulation units. Thanks to recent advances in EMS technology, portable and relatively low-cost stimulators can be purchased and used by a growing number of coaches and athletes. There are 2 main applications of EMS exercise for optimizing sport performance: the low-frequency modality, which is largely used to promote the recovery process in endurance-trained athletes, and the high-frequency mode, mainly used to improve muscle strength and power in anaerobic events. The main differences between these 2 forms of EMS are the frequency modulation (<15 Hz vs >40 to 50 Hz), the stimulus-current amplitude (submaximal and painless vs maximal and painful), and, consequently, the force produced by the muscle (<10% vs >50% of the maximal voluntary-contraction force). Despite the fact that low-frequency EMS is largely adopted by competitive endurance athletes, there is no scientific support regarding its ability to enhance the recovery process, and its presumed superiority to other methods remains to be demonstrated.1 For this reason, the effect of high-frequency EMS-induced resistance exercise (also known as neuromuscular EMS) is the focus of this technical report.
Banerjee, Prithwish, Brian Caulfield, Louis Crowe, and An- drew Clark. Prolonged electrical muscle stimulation exercise improves strength and aerobic capacity in healthy sedentary adults. This investigation evaluated training responses to prolonged electrical muscle stimulation (EMS) in sedentary adults. Fifteen healthy subjects (10 men, 5 women) with a sedentary lifestyle completed a 6-wk training program during which they completed an average of 29 1-h EMS sessions. The form of EMS used by the subjects was capable of eliciting a cardiovascular exercise response without loading the limbs or joints. It achieved this by means of inducing rapid, rhythmical contractions in the large leg muscles. A crossover study design was employed with subjects undergoing their habitual activity levels during the non-training phase of the study. The training effect was evaluated by means of a treadmill test to determine peak aerobic capacity [peak oxygen consumption (V˙ O2)], a 6-min walking distance test, and measurement of body mass index (BMI) and quadriceps muscle strength. At baseline, the mean values for peak V˙ O2, 6-min walking distance, quadriceps strength, and BMI were 2.46 ± 0.57 l/min, 493.3 ± 36.8 m, 360.8 ± 108.7 N, and 26.9 ± 3.4 kg/m2, respectively. After training, subjects demonstrated statistically significant improvements in all variables except BMI. Peak V˙ O2 increased by an average of 0.24 ± 0.16 l/min (P < 0.05), walking distance increased by 36.6 ± 19.7 m (P < 0.005), and quadriceps strength increased by 87.5 ± 55.9 N (P < 0.005); we did not observe a significant effect due to training on BMI (P > 0.05). These results suggest that EMS can be used in sedentary adults to improve physical fitness. It may provide a viable alternative to more conventional forms of exercise in this population.
TECHNOLOGIES IN MEDICINE and rehabilitation that encourage or facilitate participation in physical activity can have a beneficial effect on public health. This is especially true in the case of those who are unable to participate in physical exercise or have barriers to participation, for example those with obesity or spinal cord injury (SCI). In recent years much attention has been directed toward the use of electrical muscle stimulation (EMS) in promoting exercise. This has primarily taken the form of EMS-induced leg cycling exercise (EMS-LCE), and most research has been directed toward its use in the SCI population. Prolonged use of EMS-LCE can result in improvements of 10 –35% in aerobic capacity [peak oxygen consumption (V˙ O2)] in SCI subjects (6, 7, 9, 11).
We have developed a new approach to inducing an exercise response using EMS technology. This system is an advance on EMS-LCE as it elicits an exercise response without loading the limbs or joints, it does not involve performance of external work, and it is also very small and portable. In this approach, a series of rapid, rhythmical EMS-induced muscle contractions that mimic shivering cause a demand for oxygen in the large lower extremity muscle groups, thus resulting in a physiological response consistent with physical exercise (2). A previous investigation demonstrated that submaximal stimulation with this form of EMS results in significant increases in V˙ O2, heart rate (HR), and minute ventilation compared with resting values in healthy adults (1). Physiological responses observed were consistent with those expected in light to moderate voluntary exercise with peak EMS-induced exercise intensities ranging from 2.5 to 7.7 metabolic equivalents.
The purpose of this study was to investigate the effects of prolonged use of this form of EMS on physical fitness and body weight. We hypothesized that repeated exposure to this EMS would result in increases in cardiovascular fitness and muscle function and would bring about associated decreases in body mass in a group of sedentary adults. Our rationale was that the EMS would induce repeated rhythmical contractions of large lower extremity muscle groups and that this would bring about the following changes: 1) an improvement in exercise capacity by means of repeatedly inducing an increased oxygen demand in the tissues and therefore loading the cardiovascular system, 2) increased muscle strength by inducing repeated muscle contractions and therefore increasing the muscle mass, and 3) a reduction in body mass by means of repeatedly causing increased energy expenditure. In this first study into the prolonged effects of this form of EMS training, we have chosen to investigate its effects in a group of healthy yet sedentary adults. This population has been chosen as it is one in which exercise training is likely to be beneficial and also is one in which a training effect is more likely due to the fact that they have relatively low levels of baseline fitness. We examined peak exercise capacity, muscle strength, and body mass index (BMI) before and after a short-term EMS-induced exercise (EMS-EX) training program in healthy adults with a self-reported sedentary lifestyle.
METHODS
Twenty-two healthy adults volunteered to participate in the EMS-EX training program. The Hospital Ethics Committee approved the study, and written, informed consent was obtained in all cases. The 22 subjects included 12 men and 10 women with a mean age of 48.3 ± 12.0 yr (range 25–72 yr) and an average mass and BMI of 78.2 ± 12.2 kg and 27.1 ± 3.6 kg/m2, respectively. The subjects’ average peak V˙ O2 was 30.0 ± 6.4 ml · kg-1 · min-1. The sedentary status of the study subjects was established by means of self-report at an initial interview. None of the study subjects reported regular participation in sports, recreational activities, or training activities, and none walked or cycled to work. Prior to participation in the study, each subject completed the Physical Activity Readiness Questionnaire (14) and underwent a complete physical examination to ensure that they were fit to undertake physical activity. Physical examination was completely normal in all subjects.
Experimental design. A crossover study design was used and subjects were randomized to study groups A or B. Group A completed a 6-wk EMS-EX training program followed by a 2-wk washout period, and then a 6-wk control period during which they maintained their habitual activity level. Subjects allocated to group B underwent the same interventions in a reversed schedule, i.e., habitual activity followed by washout period followed by EMS-EX training. In all cases, measurements of exercise capacity, muscle strength, and body composition were taken at baseline, at 6 wk and at 14 wk. Subjects were not required to wear activity monitoring devices or complete habitual activity questionnaires during the study period. However, they were questioned regarding their activity levels at each measure- ment session to ensure that they did not change their habitual activity level at any stage of the study other than participating in EMS-EX exercise.
Measurements. Exercise capacity was evaluated in two ways. First, subjects completed a modified Bruce treadmill exercise test while cardiopulmonary gas exchange was simultaneously assessed. Subjects wore a facemask and a gas analysis system calibrated against gases of known concentrations according to manufacturer’s guidelines (Jaeger, Oxycon Delta) was used to measure the expired oxygen and carbon dioxide concentration and volume. V˙ O2 was calculated from these measurements. Subjects were required to walk on the treadmill at incremental velocities and inclines until any of the following end- points were reached; a leveling of V˙ O2 response despite increasing exercise intensity, abnormal cardiovascular signs, or fatigue. In all cases, in this investigation the reason for terminating the treadmill test was subject fatigue. Peak V˙ O2 and test duration were used as indica- tors of test performance. Peak V˙ O2 was calculated from the average V˙ O2 measurement during the last 30 s of the treadmill test at each test session. Subjects were also assessed using the 6-min walk distance test (4). In this test, subjects completed as many laps of a 15-m walkway as they could in a 6-min period. Subjects self-selected their walking pace and were permitted to take rests during the test period if they so wished. The distance covered during the 6-min period was taken as a measure of their functional exercise capacity.
Isometric muscle strength was assessed using a dynamometer (AFTI Torque/Force Indicator). Subjects sat in a custom-made chair with their hips and knees at 90°. Their right shin was strapped into a cuff, and they completed three maximal isometric extension holds of 5-s duration while force was measured in newtons. The maximum effort was taken as an index of maximal isometric quadriceps strength. In the case of the tests outlined above, minimal verbal encouragement was given to subjects to minimize bias as the assessors were not blinded to the subjects’ condition.
Body weight was assessed using the BMI. This was calculated from the subjects’ height (measured with SECA height monitor) and body mass (measured using Soehnle S-20 Scales). BMI is expressed in kilograms per square meter.
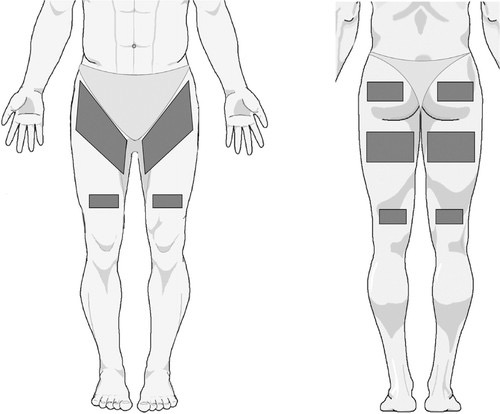
Stimulation. A specially designed handheld muscle stimulator (Bio- Medical Research, Galway, Ireland) powered by a 9-V battery was used to produce EMS-EX in this investigation. The stimulator current waveform was designed to produce rhythmical contractions in the lower extremity muscle groups occurring at a frequency of 4 Hz. The maximum peak output pulse current used in the present study was 300 mA. Impulses were delivered through five silicon-rubber electrodes on each leg (area per leg = 600 cm2) as illustrated in Fig. 1. These were applied to the body via a pair of tight-fitting shorts, which extended to the knee. This array of electrodes produced contractions in the quadriceps, hamstrings, gluteal, and calf muscles.
Study procedure. A training schedule and exercise prescription was given to all subjects during the 6-wk EMS-EX training phase of the study (Table 1). Subjects were requested to complete five 1-h training sessions per week at times of their own choosing in their own homes. The first and last 10 min of training sessions consisted of gradual warm-up and cooldown periods. This was achieved by means of gradually increasing or decreasing the output intensity of the stimu- lator as appropriate. For the remaining 40-min period, subjects were requested to set the stimulator to their target training intensity, which was arrived at by means of a combination of their subjective percep- tion of their work rate and their heart rate (HR) response to stimula- tion. The subjects were told to attempt to work at their maximal subjective work rate with the proviso that their HR did not rise above the 90% limit of their HR reserve. Subjects were given an individu- alized exercise prescription with their own HR limit for exercise and were required to wear HR monitors during each session. Subjects were required to complete a training log in which they recorded the output intensity of the stimulator and their maximal HR reached during each session. During the control phase of the study, subjects were asked not to undertake any exercise above and beyond their habitual exercise level.
Six subjects dropped out during the course of the study. We observed no gender or age bias in the subjects who dropped out of the study. The reasons for dropout included chest infection/cold (2 sub- jects), knee pain (1 subject), unable to tolerate EMS (2 subjects), and no show after baseline testing (1 subject). A additional two subjects completed the trial yet were excluded from analysis due to interrup- tion to training schedule due to death of family member (1 subject) and self-reported increase of habitual activity level during the control leg of the study (1 subject). A further two subjects were excluded from analysis of treadmill test results due to technical problems encoun- tered during testing.
Due to these dropouts/exclusions, there were a total of 15 subjects (10 men, 5 women) included in the final analysis of BMI, muscle strength, and walking distance results, whereas 13 subjects (8 men, 5 women) were included in the analysis of treadmill test results. Of the
15 subjects, 9 were randomized to group A and 6 to group B. Log sheets returned by these subjects indicated that their self-reported level of compliance with the training program was very good, with an average of 29 exercise sessions completed.
Data analysis. Each subject underwent baseline testing followed by 6 wk of EMS-EX training and 6 wk at their habitual exercise level (control) during the study. Thus subjects acted as their own control for the purposes of statistical analysis. Responses of all measured vari- ables to EMS-EX training and the 6-wk control period were assessed using the following data groupings: EMS-EX response consisted of group A measurements at 6 wk and group B measurements at 14 wk, whereas control response was calculated from group A measurements at 14 wk and group B measurements at 6 wk. Differences in the measured variables under each of the three conditions, baseline, EMS-EX response, and control response, were first compared using repeated-measures ANOVA. Post hoc paired t-tests were subse- quently used to compare differences between baseline and EMS-EX response, between baseline and control response, and between EMS-EX and control response. The level of significance was set at P < 0.05. The relationships between changes in measured variables after EMS-EX training and both baseline values and relative physiological intensity of the EMS-EX training were analyzed by means of calculating the Pearson’s product-moment correlation coefficient (r) and its square (r2).
RESULTS
Group mean (±SD) values for each of the measured variables representing baseline values and EMS-EX and control responses are detailed in Table 2. Repeated-measures ANOVA testing demonstrated that there were highly significant within-subjects effects for condition when baseline, EMS-EX response, and control response were compared. We subsequently carried out post hoc comparisons between conditions using two-sided paired t-tests (Table 3). This analysis revealed that there were no significant differences between baseline values and control response for treadmill walking time, peak V˙ O2, 6-min walking distance, and quadriceps strength (P > 0.05). There were, however, significant differences between baseline and EMS-EX response, and between EMS-EX response and control response for all these variables. The EMS-EX responses were significantly higher (P < 0.05), indicating the presence of a significant treatment effect for these variables. When comparisons were made across conditions for BMI, we did not observe a treatment effect. Post hoc comparisons revealed small yet significant differences between EMS-EX and control responses and between baseline and control response, yet not between baseline and EMS-EX response. When we analyzed the relationship between baseline values for the measured variables and the percent change in these variables after EMS-EX training, we did not observe any strong relationships (Table 4). The strongest relationship observed was that between baseline peak V˙ O2 and percent change in peak V˙ O2 after EMS-EX training (r = -0.62, r2 = 0.38), suggesting only a moderate relationship. EMS-EX training log sheets were completed by 13 of the 15 subjects who finished the study. Averaged data from these log sheets indicated that subjects used the stimulator at 46.3 ±
13.0% of its maximum output during training. This was associated with a training HR response (HRR) of 98.0 ± 11.6 beats/min, corresponding to 56.8 ± 10.2% of subjects’ maxi- mum HR (from their baseline treadmill test). We observed little relationship between the relative physiological intensity of the EMS-EX training and the percent change in measured variables after EMS-EX training. This weak relationship was similar whether we used HR response during EMS-EX training or HR response as a percentage of maximum HR during EMS-EX training as our indicator of the relative physiological intensity of EMS-EX (Table 5).
DISCUSSION
The principal finding from this investigation was that a group of sedentary adult subjects demonstrated significant improvements in exercise capacity (including cardiovascular fitness and muscle strength) as a result of a period of EMS-EX training. This is the first study to demonstrate that such an effect is possible with use of a form of EMS that does not involve loading of the limbs or joints and that does not involve performance of external work.
The baseline cardiovascular fitness profile of the subjects tested in this study was similar to that expected in untrained adults (8). The male subjects demonstrated lower mean baseline 6-min walking distance scores than population norms (501 vs. 576 m), whereas female scores were in line with population norms (494 vs. 494 m) (4). These findings, along with the fact that average baseline BMIs were in the overweight range, suggested that the general physical fitness and body mass profile of the subjects in the present study was consistent with that of a sedentary, untrained adult population.
The EMS-EX stimulation was generally well tolerated by subjects with a good level of compliance. However, we relied on self-reported compliance to measure adherence to the training program. This may have resulted in an overstating of the actual frequency of training sessions undertaken by subjects. Shankar and coworkers (13) reported that self-reported adherence and objectively measured evidence of adherence might vary in up to 50% of subjects. The majority of subjects selected a stimulation intensity that was sufficient to produce a HRR in their training zone. The average EMS-EX HRR, 57% of maximum HR, is consistent with the lower end of the training intensity zone recommended by the American College of Sports Medicine (55–90% of maximum HR) (12).
Increases of 10% were observed in peak V˙ O2 and treadmill test duration after EMS-EX training in this study. Engaging in any mode of exercise at the training intensities observed in this study could be expected to produce moderate increases in cardiovascular fitness in a sedentary adult population. However, we also observed increases in 6-min walking distance (7.5%) and muscle strength (25%). This suggests that this mode of training has good carryover to other components of physical fitness.
The precise mechanism underlying observed improvements cannot be ascertained from the data obtained in the present study. The improvement in muscle strength may have been achieved through increase in muscle bulk as a result of repetitive contractions. It may also have arisen from facilitation of spinal motor neuron pools via stimulation of afferent pathways, increased sensitivity of neural synapses, and better synchronization of motor unit firing patterns. The selective recruitment of large fast-twitch type II fibers over the slow-twitch type I fibers could also be implicated (3). The improvement in whole body performance may have involved a central contribution, but we believe that improved ergo reflex activity, as we have previously shown in a heart failure population using arm exercise (10), is important too.
We did not observe any significant changes in BMI in our subjects after EMS-EX training. There was a small yet significant decrease in BMI when control and EMS-EX responses were compared, yet there was no difference between EMS-EX response and baseline. This is not a surprising result as we did not control for other factors that may influence body weight during our study period, such as food intake. It would be useful to examine the effect of this form of exercise on body weight in future studies carried out over longer periods with good control over other influencing factors.
One of the advantages of this mode of training is that subjects were able to demonstrate improvements in a wide range of physical fitness variables without loading their limbs or joints.
This suggests that this form of exercise could be suitable for subjects in whom repeated weight bearing could exacerbate degenerative joint conditions, such as osteoarthritis. In addition, although EMS-EX is associated with and will be limited by perceived exertion on behalf of the individual undertaking the exercise, no voluntary effort is required to participate in this form of exercise. The work is created by means of EMS-induced muscle contractions. It is reasonable to expect that the improvements seen here in sedentary untrained adults could also be achieved in populations unable to engage in voluntary exercise such as those with SCI or obesity.
Our subjects demonstrated moderate increases in peak V˙ O2, 10%. Improvements of up to 35% in peak aerobic capacity have been reported in SCI subjects using EMS-LCE (7). However, baseline peak V˙ O2 levels in the subjects in the current investigation, averaging 2.45 l/min, were much higher than those of subjects in previous investigations, which aver- aged 1.0 –1.5 l/min (7, 9). Therefore, the scope for improvement was greater in previous investigations. Additionally, our subjects were limited by their sensory feedback while using the stimulator. They used the device at stimulation intensities that were within the limits of their comfort zone. SCI subjects would be able to tolerate far higher stimulation intensities and therefore could train at a higher percentage of maximum HR using this form of stimulation.
A limitation of this study lies in the fact that we are unable to make strong conclusions regarding the relationships between baseline status and relative physiological intensity of EMS-EX and the level of change in measured variables after EMS-EX training. This is due to the small sample size in this study and the relative similarity in fitness profile of our subjects. Our data indicated that �40% of the change in peak V˙ O2 could be attributed to baseline status. However, it is reasonable to expect that greater improvements would be observed in our subjects than would be seen in a population of highly trained athletes. We failed to identify any relationship between physiological responses during EMS-EX and the degree of change in any of our measured variables. We cannot rule out the possibility that subjects made errors during monitoring or recording their HR during training, so these results should be interpreted with caution. In a previous study we demonstrated that a clear dose-response relationship exists between the stimulation intensity and immediate physiological response (measured using V˙ O2, carbon dioxide production, minute ventilation, and HR) with this form of EMS (1). If this form of exercise is to develop any more, the relationship between training stimulus and outcomes requires careful investigation in further studies.
This form of exercise is not likely to be suitable for all individuals as many individuals find EMS in general difficult to tolerate. Indeed, two subjects in this present study were unable to tolerate the sensation of the EMS-EX. However, most subjects tolerated it quite well. There is still much scope for improvements in this form of EMS in terms of comfort levels due to stimulation. In addition, further research is required to determine the most effective methods of use of this technology and to identify the populations in which it is most beneficial. Despite this, the results of this first investigation into the effects of prolonged exposure to this form of exercise are very encouraging. We demonstrated that improvements in physical fitness are associated with unloaded EMS-induced muscle contractions. Additional improvements to this technology could result in it becoming a very important clinical tool in health and fitness promotion in the future.
REFERENCES
1. Banerjee P, Caulfield B, Crowe L, Witte K, and Clark AL. Electrical stimulation of unloaded muscles causes cardiovascular exercise by in- creasing oxygen demand. Eur J Cardiovasc Prevention Rehab In press.
2. Caulfield B, Crowe L, Minogue C, Banerjee P, and Clark A. The use of electrical muscle stimulation to elicit a cardiovascular exercise response without joint loading: a case study. J Exercise Physiol Online 7: 84 – 88,
2004.
3. Delitto A and Snyder-Mackler L. Two theories of muscle strength augmentation using percutaneous electrical stimulation. Phys Ther 70:
158 –164, 1990.
4. Enright PL. The six-minute walk test. Respir Care 48: 783–785, 2003.
5. Enright PL and Sherrill DL. Reference equations for the six-minute walk in healthy adults. Am J Respir Crit Care Med 8: 1384 –1387, 1998.
6. Goss FL, McDermott A, and Robertson RJ. Changes in peak oxygen uptake following computerised functional electrical stimulation in spinal cord injured. Res Q Exerc Sport 63: 76 –79, 1992.
7. Hooker SP, Figoni SF, Rodgers MM, Glaser RM, Matthews T, Surya- prasad AG, and Gupta SC. Physiologic effects of electrical stimulation leg cycle exercise training in spinal cord injured persons. Arch Phys Med Rehabil 73: 470 – 476, 1992.
8. McArdle WD, Katch FI, and Katch VL. Exercise Physiology: Energy, Nutrition, and Human Performance. London: Lippincott Williams & Wilkins, 2001.
9. Mutton DL, Scremin MD, Barstow TJ, Scott MD, Kunkel CF, and Cagle TG. Physiologic responses during functional electrical stimulation leg cycling and hybrid exercise in spinal cord injured subjects. Arch Phys Med Rehabil 78: 712–718, 1997.
10. Piepoli M, Clark AL, Volterrani M, Adamopoulos S, Sleight P, and Coats AJS. Contribution of muscle afferents to the hemodynamic, auto- nomic and ventilatory responses to exercise in patients with chronic heart failure: effects of physical training. Circulation 93: 940 –952, 1996.
11. Pollack SF, Axen K, Spielholz N, Levin N, Haas F, and Ragnarsson KT. Aerobic training effects of electrically induced lower extremity exercise in spinal cord injured people. Arch Phys Med Rehabil 70: 14 –21,
1989.
12. Pollock ML, Gaesser GA, Butcher JD, Despres JP, Dishman RK, Franklin BA, and Ewing-Garber C. The recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness and flexibility in healthy adults. Med Sci Sports Exerc 30:
975–991, 1998.
13. Shankar K, Mihalko-Ward R, Rodell DE, Bucher A, and Maloney FP.
Methodologic and compliance issues in postcoronary bypass surgery subjects. Arch Phys Med Rehabil 71: 1074 –1077, 1990.
14. Thomas S, Reading J, and Shephard RJ. Revision of the Physical
Activity Readiness Questionnaire (PAR-Q). Can J Sport Sci 17: 338 –345,